Myths about will power and moral weakness keep people with opioid use disorder from receiving effect
Prescription medications can help people with opioid use disorder avoid the risks of relapse and overdose. But stigma based on misperceptions about addiction limits their use.


The most effective science-based treatment for opioid use disorder is medication. Methadone and buprenorphine prevent intense cravings and other symptoms of withdrawal, while naltrexone works by blocking the effects of opioids.
Despite abundant research showing these medications reduce the risk of relapse and overdose, many people, no matter their relationship with opioids or with people who use them, are still hesitant to support the use of these medications. And the majority of people who would benefit from such treatments do not have access to them.
We study opioid use disorder and the attitudes that surround it. To better understand hesitancy around the use of medication to treat opioid use disorder, we and our colleagues conducted focus groups with three populations intimately involved in the opioid crisis – those in recovery, their friends and family and their health care providers – as well as with community members with no direct connection to opioid use disorder. We spoke with 101 people in all across rural and urban locations in Indiana.
We asked what they thought about using medication to treat opioid use disorder. We found all four groups had negative opinions about using medication. No matter who they were, participants voiced an underlying belief that opioid use disorder results from moral weakness that can be overcome with willpower and commitment to behavior change, despite research-based evidence that overwhelmingly shows that opioid use disorder is a chronic brain disease best managed with medication.
Across all four groups, we heard three myths about using medication for opioid use disorder. Research reveals these stigmatizing beliefs are counter to reality.
Medication isn’t trading one drug for another
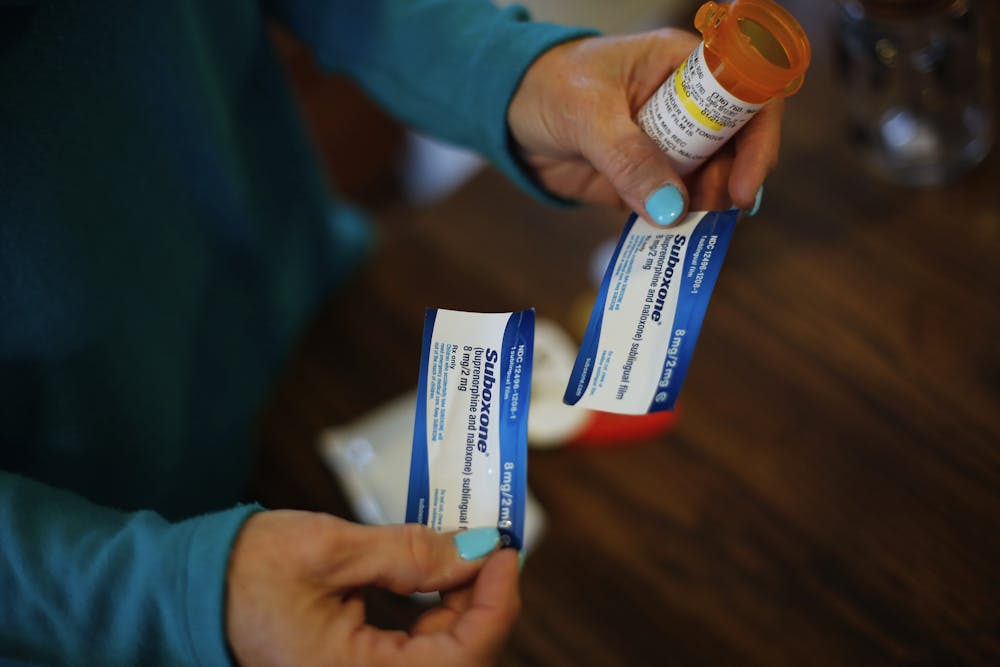
Many of our participants expressed the belief that using medication is the same as using opioids to get high. This misperception is likely rooted in the outdated idea that recovery is defined by total abstinence from all substances, except perhaps caffeine and nicotine. As one service provider working with people in recovery declared, “If you’re on Suboxone or you’re on methadone and you’re not being tapered down, you’re using.”
The truth is, taking medication is not the same as using prescription or street opioids to get high. These medications do not produce the same experience of euphoria or high as heroin, morphine or other opioids. In different ways, methadone, buprenorphine and naltrexone all reduce cravings and allow people to remain sober and to work, raise their children and engage in activities of healthy productive living – all challenges for people to do well when using opioids to get high.
Medication is an important part of long-term recovery
We found that people’s overall discomfort with the idea of using medication to treat opioid use disorder led to a belief that such treatment should be used only as a steppingstone on the way to sobriety. A community member we spoke with said, “It’s a way of weaning them off everything. I think that’s just one of the steps they have to take to get clean.”
The belief that medication should be used for only a short time runs counter to research showing higher rates of relapse after tapering. Guidelines from the U.S. Department of Health and Human Services discourage rapid tapers and affirm that long-term use is the best way to prevent relapse, overdose and death.
Long-term treatment counts as success
Many of our study participants voiced the belief that long-term use of medication means the treatment did not work. As one family member put it, “If you’re on it for 10 or 15 years, then that’s not really helping you.”
The myth that long-term use of medication means the medicine is ineffective – or has failed – runs counter to both the life outcomes of those on maintenance treatment and the physiological reality that such drugs may remain necessary to normalize brain function for the person in recovery.
Just as those with high blood pressure or diabetes may need to remain on medications for the long term, so might some people with opioid use disorder. Keeping people in treatment and alive through use of medications is treatment success, not failure.

An estimated 3 million Americans have had or currently struggle with opioid use disorder. The latest data from the U.S. Centers for Disease Control and Prevention estimates nearly 83,000 deaths in 2022 involved opioids.
Methadone, buprenorphine and naltrexone are lifesaving medications. Myths associated with their use cause avoidable relapse, overdose and death by keeping people from using the most effective tool for entering into and maintaining recovery.
Melissa S. Fry receives funding from Indiana University Addictions Grand Challenge Program, and provides evaluation services to Substance Abuse and Mental Health Services Administration funded programs.
Melissa Cyders receives funding from Indiana University Addictions Grand Challenge Program and the National Institutes of Alcohol Abuse and Alcoholism.
Read These Next
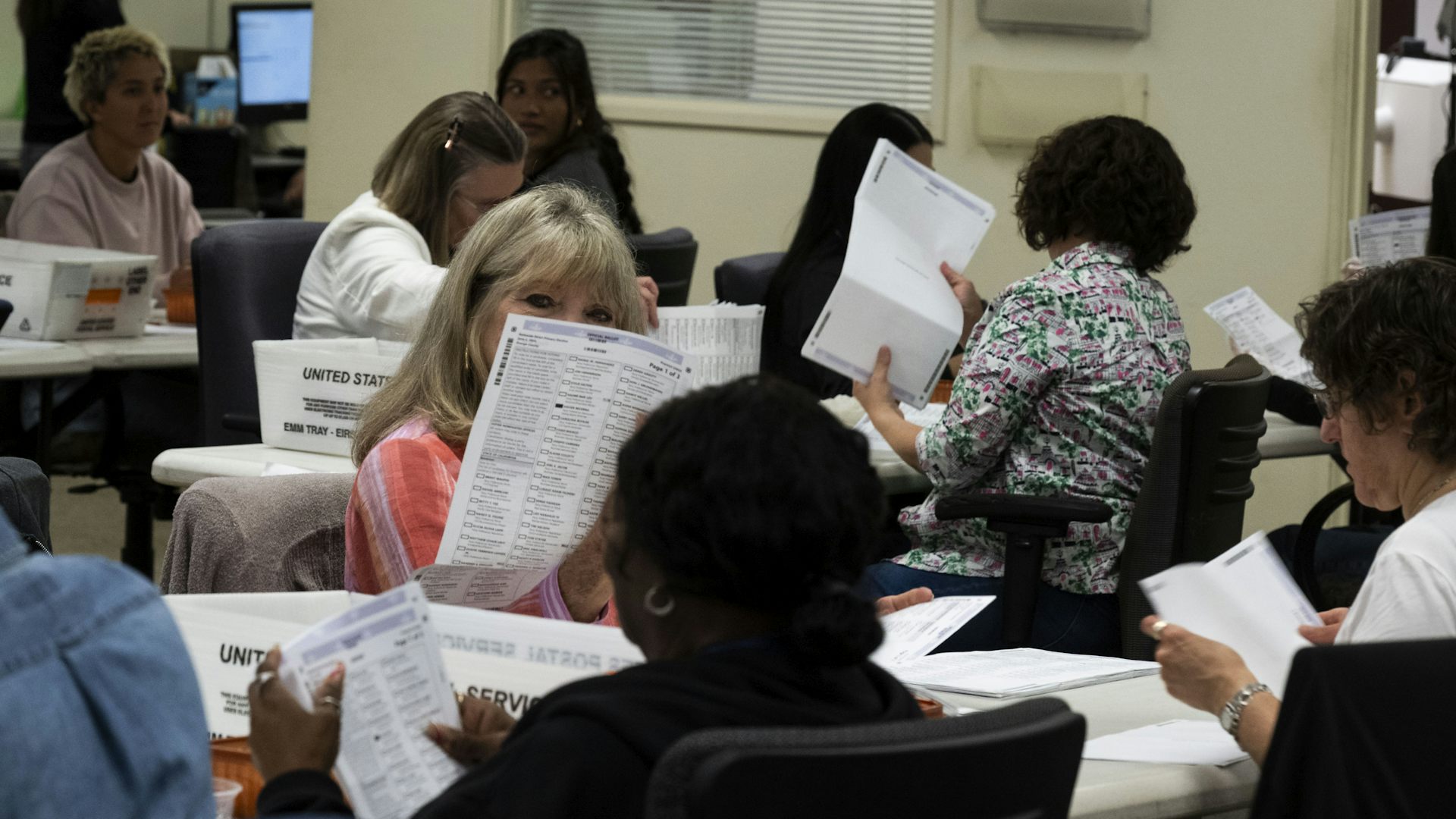
Mail-in voting: Trump administration appeals to Supreme Court to revive executive order setting limi
The U.S. Constitution gives states control of elections. An executive order by President Donald Trump…

How the Trump administration’s rhetoric promotes anti-transgender views
How invented threats, provocative language and repulsive imagery contribute to declining support for…

Trump administration changes to ‘public charge’ rule could keep millions of immigrants – and their U
A new policy could deny an immigration application based in part on the use of government benefits by…

